Customer Support
888-STATEFUND (888-782-8338)
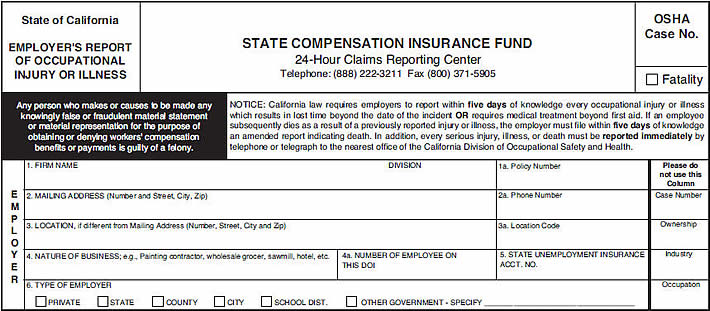
Enter company name as indicated on your Annual Rating Endorsement or policy.
DIVISION
If applicable, provide the specific department or division where injury occurred.
Include the group & policy number, or policy number with current year, separated with dashes or spaces. For example: 673-45-10 (group-policy number-policy year) or 1834567-10 (policy number–policy year).
Use the address shown on your Annual Rating Endorsement or policy.
Provide your company’s primary contact phone number, including area code.
Indicate the physical address of where the injury occurred, including street address, suite # (if applicable), city and ZIP code.
If applicable, use the code corresponding to the location, department, or division where the injury took place.
Provide a general description of your business.
The total number of employees working on the date of injury.
Enter your State of California Unemployment Insurance account number, also known as your “State Tax ID Number” or “EDD Number” (Employment Development Department).
Place a check mark or “x” on the box that best describes your business (private, state, county, city, school district, other government).
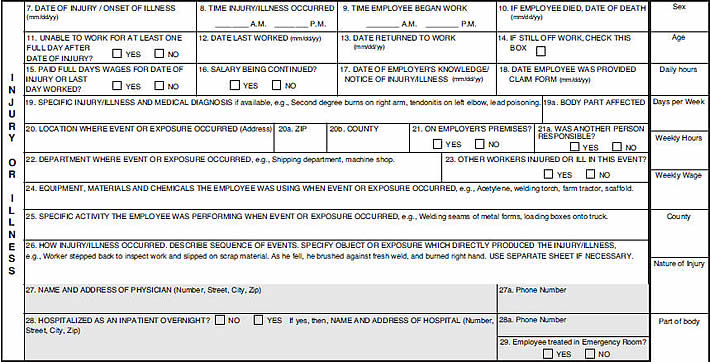
For specific injuries (such as slip & fall), use the actual date when the incident happened. For injuries or illnesses that are results of exposure to continuous trauma, chemicals, stress, etc., over time, the appropriate date to use would be:
Enter the actual or approximate time when the injury happened. You may also use “unknown” if applicable.
Enter the time the injured worker started his/her shift on the day of injury/illness.
Enter date of death if the worker died as a result of his/her injuries/illness.
Choose “Yes” if the injured worker has missed one full day or more of work because of the injury.
Enter the date that the injured worker last worked (month, day, year).
Enter the date the injured worker returned to work, if applicable (month, day, year). Leave blank if the injured worker has not yet returned to work, and check box 14.
Check box if the injured worker is still off work at the time of this report’s completion.
Check “Yes” if you paid the injured worker for a full day or “No” if you only paid for the hours worked.
Indicate here if the injured worker receives tips, overtime pay, meals, or other non-wages.
Indicate the date you were first notified or became aware of the injury or illness (month, day, year). Please do not leave blank.
Enter the date you provided the injured worker with the employee claim form (month, day, year).
Provide details about the worker’s injury/illness. Be specific as to which body part was affected and the type of injury.
Enter the actual physical location where the injury occurred (street address, suite # (if applicable), city, ZIP code). If the injury happened at a job site, indicate that location’s address. If specific information is not available, enter “job site – address unknown.”
Enter the County name where the injury occurred.
Check “Yes” if the injury occurred at your business location, or “No” if it occurred at a job site, public road, or other venue away from the main business location.
Check “Yes” if another person was directly or indirectly responsible for the injury.
Enter the specific business location, such as warehouse, assembly area, kitchen, garage, or other work area.
Check “Yes” if more than one employee was injured in this single occurrence or incident.
Detail any equipment, materials or chemicals the injured worker was handling or exposed to at the time of injury or illness.
Briefly state what the injured worker was doing at the time of injury.
Describe how the injury or illness occurred, providing as many details as available.
Enter the complete information for the doctor or medical facility providing the initial medical evaluation or treatment (first and last name, facility name, street address, suite # (if applicable), city, ZIP code).
Enter the treating doctor or medical facility telephone number, including area code.
Check “Yes” if the injured worker was hospitalized overnight; provide hospital details if applicable (name, street address, city, ZIP code).
Enter the phone number of the admitting hospital, including area code.
Check “Yes” if the injured worker received initial treatment in the emergency room.
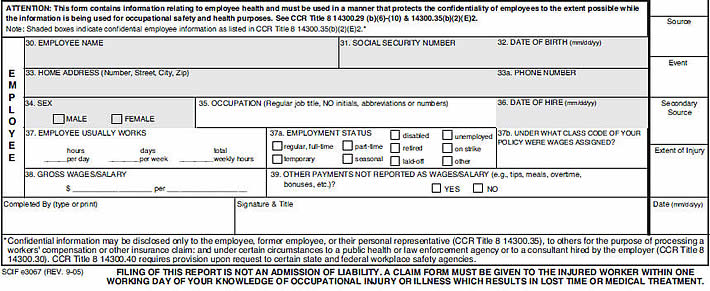
Enter the injured worker’s complete legal name (first, middle, last).
Enter the injured worker’s social security number.
Enter the injured worker’s complete date of birth (month, day, year).
Injured worker’s complete home address, including street address, apt. # (if applicable), city and ZIP code.
Enter the injured worker’s home phone number, including area code.
Enter the injured worker’s gender.
Enter the injured worker’s job title or field of work.
Enter the date when the injured worker started working for your company (month, day, year).
Enter the injured worker’s regular or average hours worked.
Enter the injured worker’s employment status at the time of injury (regular, full-time, part-time, temporary, seasonal, disabled, retired, laid-off, unemployed, on strike, other).
Enter the injured worker’s employee class code (as used for payroll) at the time of injury.
Enter the injured worker’s gross wages paid per week, month, or year.
Indicate here if the injured worker receives tips, overtime pay, meals, or other non-wages.
*** Please remember to include your name, title, date, and signature to complete this process. ***